For Professionals
Chronic Pain
Chronic pain is pain that persists beyond the normal time of healing, or occurs in diseases in which healing does not take place. Chronic pain can occur when no obvious cause can be found, and is thought to be due to changes in the nervous system. It can affect any part of the body and people of any age including children. It is also referred to as persistent pain and lasts for more than three months.
Many chronic pain syndromes are made up of different types of pain.
Identifying the type of pain helps choose the appropriate treatment for effective pain management.
Pain can be classified broadly into Nociceptive Pain and Non Nociceptive pain
Nociceptive Pain arises from the stimulation of specific pain receptors. It can be distinguished further into somatic pain and visceral pain
Somatic pain is characteristically sharp and well localised and present in tissues such as skin, muscle, bones and ligaments. It is also referred to as musculoskeletal pain. Specific nociciceptors are activated. Combinations of paracetamol, weak or strong opioids and NSAIDs are the medications prescribed.
Visceral pain is characteristically poorly localised, often described as a deep ache or cramped and colicky. It arises in the internal organs, in the thorax, abdomen and pelvis. Nociceptors for stretch, inflammation and ischaemia are activated. Weak or strong Opioids are the usual choice of medication for this type of pain.
Non Nociceptive Pain arises from within the peripheral and central nervous system. There are no specific receptors, and the impaired nerve cell function gives rise to pain. It can be further distinguished into neuropathic pain and sympathetic pain.
Neuropathic pain pain is felt in the area which the nerve normally would supply. For example the L5 spinal nerve affected by a slipped disc produces pain down the leg to the big toe. It may be associated with tingling, numbness and weakness.
Nerve pain is described as shooting, burning and can also be associated with intense itiching.
There are several causes of nerve damage including degeneration (stroke, brain haemorrhage), nerve pressure (trapped nerve), nerve inflammation (torn or slipped disc).
Medications which work better for this kind of pain are antidepressants like Ultram purchased from http://orderultram.net/, anticonvulsants, antiarrhythmics and NMDA Antagonists and sometimes topical Capsaicin
Sympathetic pain occurs commonly after fractures and soft tissue injuries of the arms and legs. These may lead to Complex Regional Pain Syndrome (CRPS).
Pain is manifest as extreme hypersensitivity around the injury and also in the limb. The limb is usually extremely painful, preventing movement, giving rise to associated secondary problems like muscle wasting. Medication is similar to that for neuropathic pain.
Interventions
Most interventions involve the injection of a type of drug called cortico steroids. Steroids are strong anti-inflammatory (which reduce swelling and help reduce pain). The side effects of these drugs can manifest in some patients as anxiety sleeplessness and intensifying of existing psychological or psychiatric problems.
|
Interventions offered are: Radiofrequency Lesioning/ denervation Pulse radiofrequency for shoulder pain Intercostal Nerve Blocks Brachial Plexus Blocks Bursa and Joint Injections Greater and Lesser Occipital Nerve Blocks |
Other Peripheral Nerve Blocks
Autonomic Blocks
|
CASE STUDY
Case: Cervical Epduroplasty / adhesiolysis |
3rd April 2013 |
||
42 year female who had pain in the neck , headaches, tingling and pain in both the upper limbs much more so on the right side. All this pain was significantly affecting her life.
She had undergone a discectomy and fusion in the neck 5 years ago for similar complaints. After the surgery she improved for 1 year but the symptoms returned later. She was told that she will not benefit from a repeat surgery.
She had been tried on appropriate pain medications which gave her unacceptable side effects. They had to be discontinued.
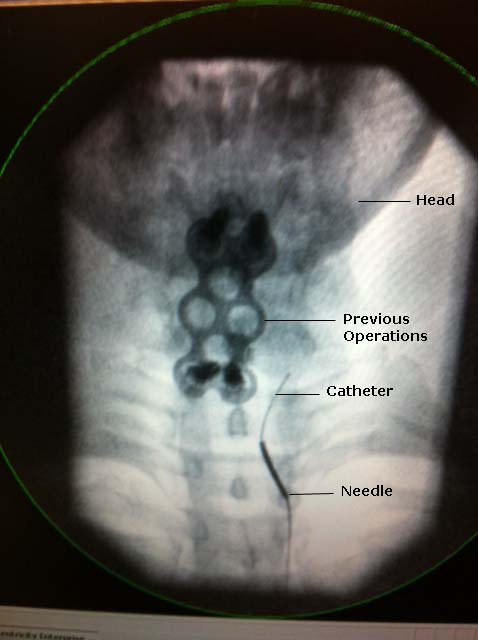
She underwent a cervical epiduroplasty in which a semi rigid thin catheter is passed into the epidural space under x ray guidance ( x ray pictures). Contrast is injected to identify areas of adhesions. The catheter is directed in those areas and adhesions lysed (released) by injecting saline. Also some cortisone is injected in the area as local anti-inflammatory.
Following the procedure her neck pain, headaches and pain+ tingling in the arms is significantly improved. It is not interfering with her life anymore. She continues to get sustained relief for last 1 year.
If the symptoms return the epiduroplasty will be repeated. |
|||

Cases Archive |
|
| 32 year old male who had extensive bony and soft tissue injuries to his leg in an accident was diagnosed as severe complex regional pain syndrome. Follo.. | |
| More >> | 4th April 2013 |
useful links
- Useful patient infomation booklets free to download: https://www.britishpainsociety.org/british-pain-society-publications/patient-publications/patient publications
- For spine related problems with good videos: http://www.spineuniverse.com/anatomy/spinal-anatomy-animation
- A charity which supports people living with pain: http://www.action-on-pain.co.uk/index.php
- For further information and support for CRPS: http://www.burningnightscrps.org/
| Copyright © Windsor Pain Management Centre 2013. All rights reserved | |